Dissociation,
Explained.
Basics of Dissociation
Dissociation refers to a disruption or disconnection in the normal integration of consciousness, memory, identity, emotion, perception, and body awareness. Rather than experiencing thoughts, feelings, and sensations as connected and continuous a person may feel separated from themselves, their surroundings, or their experiences. It exists on a spectrum, from very common, everyday experiences to more complex clinical presentations.
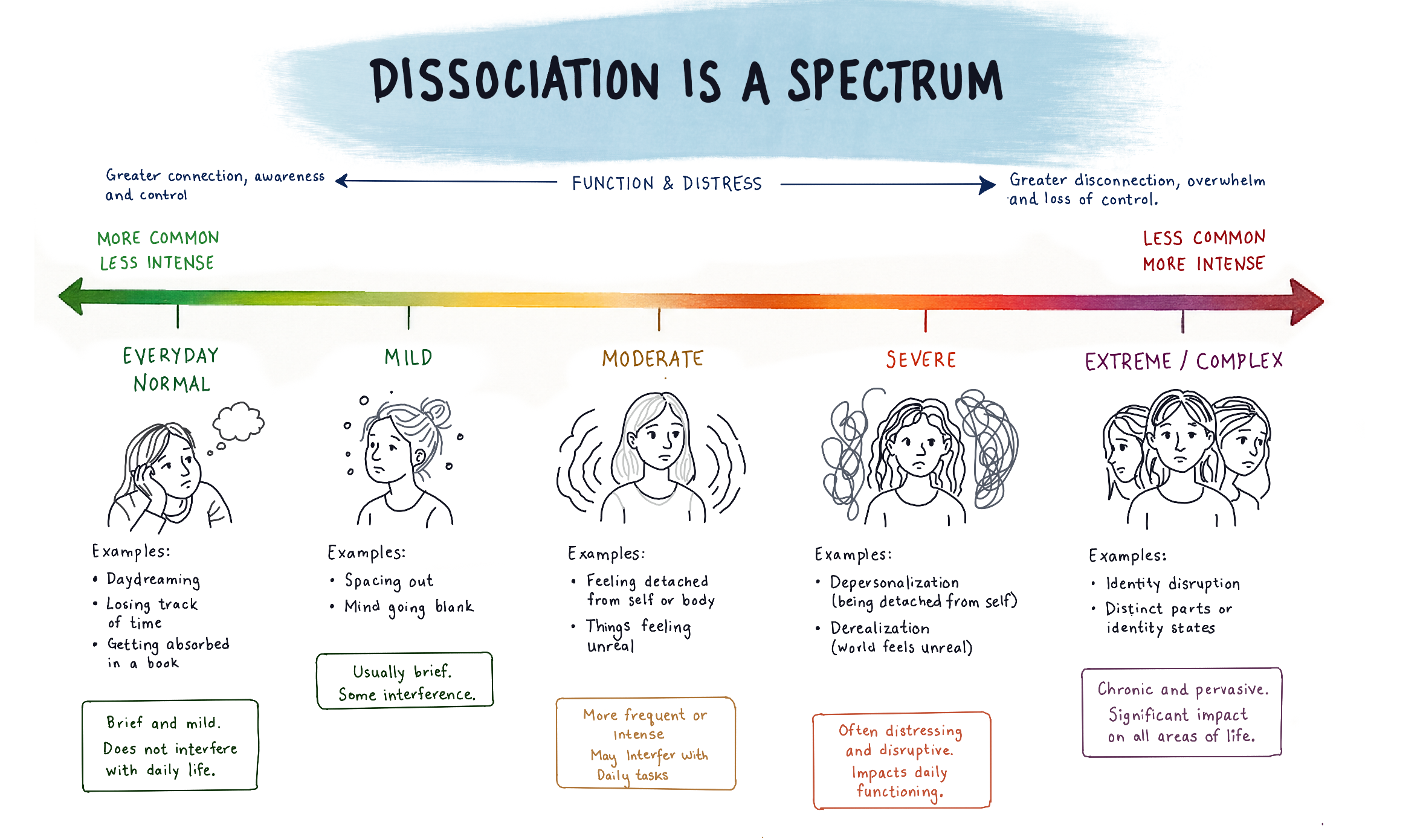
Everyone experiences dissociation to some degree, common examples include daydreaming or “spacing out.” Dissociation can also occur in response to highly stressful or potentially traumatic experiences. When these episodes happen frequently or cause significant distress or impairment, they may meet the criteria for a diagnosable dissociative disorder.
Dissociative Disorders
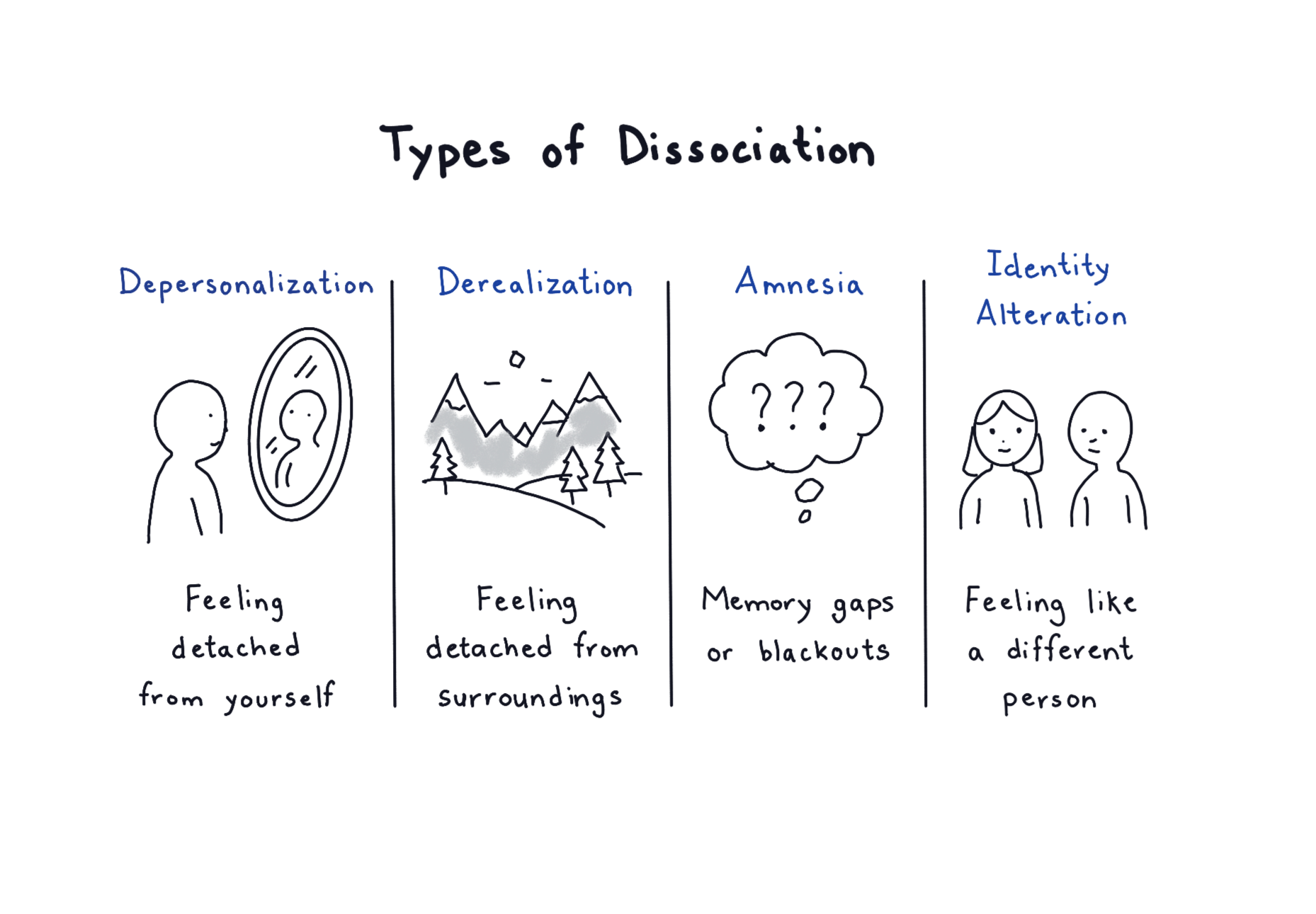
Dissociative disorders are a group of mental health conditions which involve disruptions in a person’s sense of identity, memory, consciousness, or perception. These conditions are often linked to overwhelming stress or trauma, and dissociation can function as a way for the mind to cope by creating psychological distance from the experiences. Common types of dissociative disorders include dissociative amnesia, depersonalization/derealization disorder, and dissociative identity disorder.
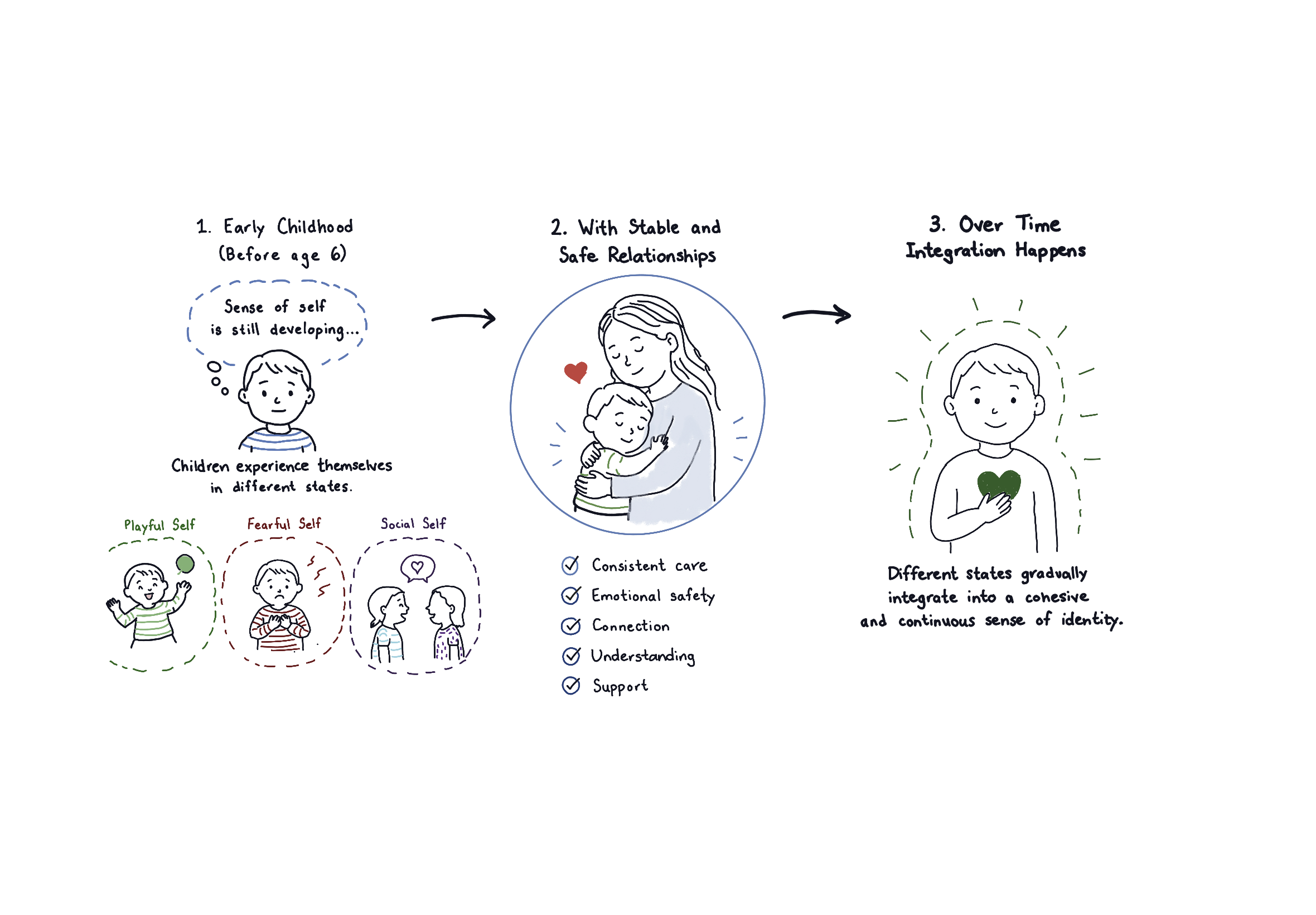
In early childhood, typically before the age of 6, a child’s sense of self is still developing, because of this children experience themselves in state-dependent ways, shifting between different emotional, behavioral, and relational “selves” (e.g., playful, fearful, social) without a stable, integrated identity.
Developmental research describes how this is normal and expected process as the neural systems responsible for autobiographical memory, self-representation, and emotional regulation, particularly within fronto-limbic networks, are still maturing.
Because of this, dissociation in childhood is relatively common and often reflects an adaptive capacity to move between states rather than a pathological process. Over time, and within the context of consistent, safe, and attuned caregiving relationships, these discrete states become increasingly linked and integrated, resulting in a more cohesive, continuous sense of self.
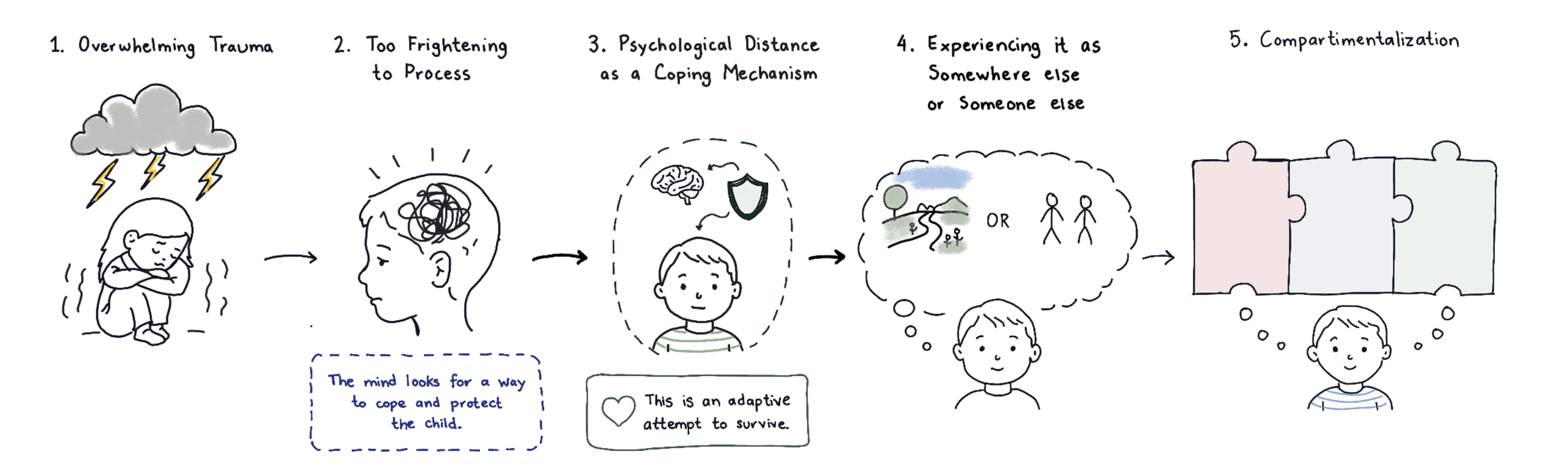
While dissociation is a normative part of early development, it can take on a different role in the context of overwhelming or chronic stress. When a child’s environment lacks sufficient safety, consistency, or attuned caregiving, the natural capacity to shift between states may be used as a primary means of coping. In this context, dissociation functions as an internal form of escape or emotional regulation, allowing the child to psychologically distance from experiences that are too intense to process or integrate. Over time, however, these state-dependent experiences may remain less connected rather than becoming integrated, particularly when stress is ongoing or relational support is limited. This can contribute to more persistent patterns of dissociation and, in some cases, the development of a diagnosable dissociative disorder.
It is also important to note that exposure to stress or trauma alone does not determine outcome. Not all individuals who experience adversity develop dissociative disorders. Research suggests that individual differences, including biological sensitivity to stress, temperament, and neurobiological vulnerability to dissociation, interact with environmental factors to influence risk. As a result, some individuals may be more likely to rely on dissociation during distress, increasing the likelihood that this adaptive process becomes more ingrained over time.
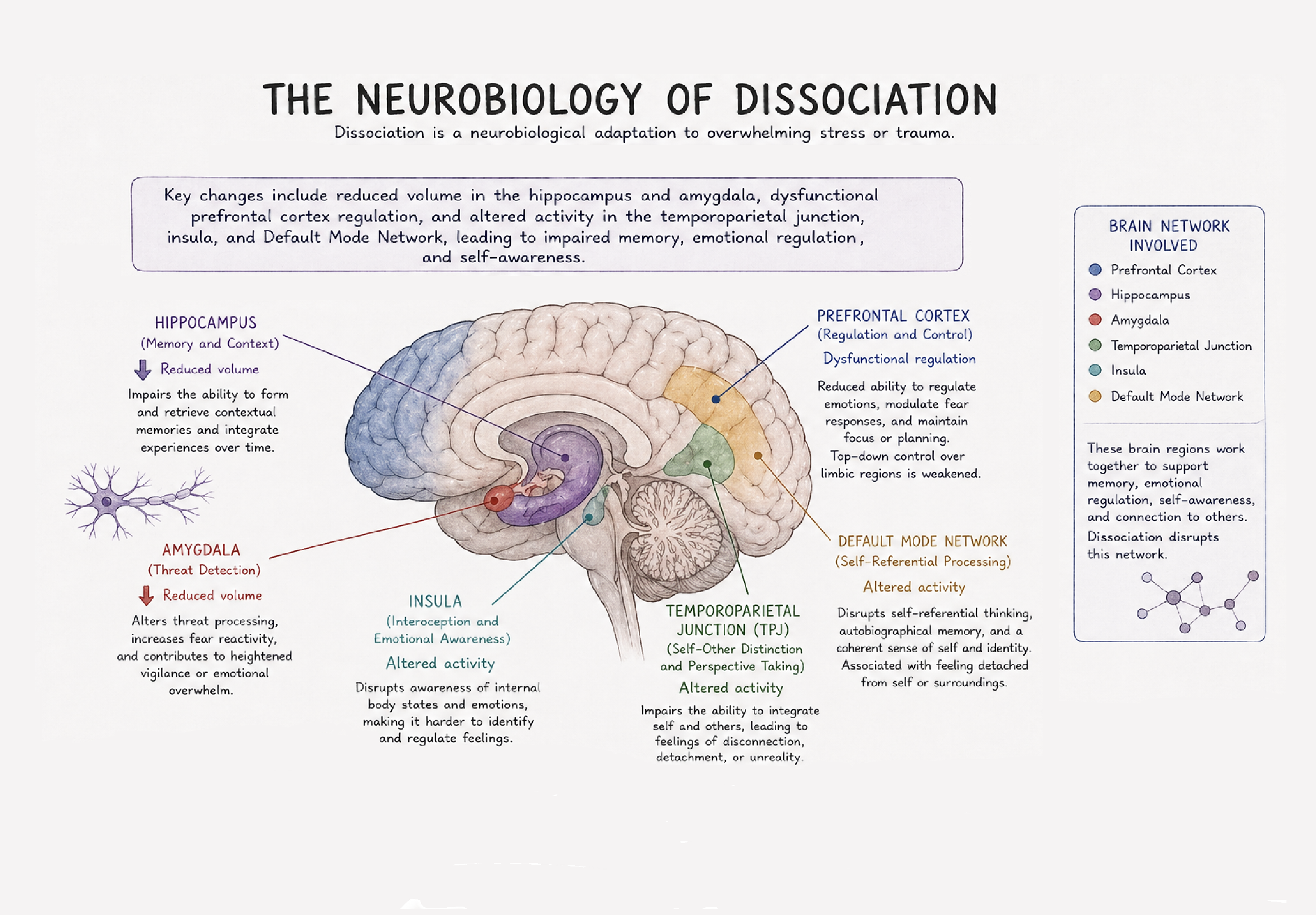
The neurobiology of dissociation is best understood as a pattern of altered coordination between brain systems involved in threat detection, emotional regulation, memory, and self-processing. Dissociation reflects how these brain networks interact under stress, and this is especially true when the stress is overwhelming or inescapable.
The threat system, which includes the amygdala, thalamus, hypothalamus, and hippocampus are responsible for activating the body’s stress response when a perceived danger is detected. In typical fear responses, this system works to prepare the body to escape the threatening situation by releasing stress hormones (e.i., cortisol, epinephrine, and norepinephrine) which causes a physiological respond that produces the “fight or flight” response. In dissociation, this pattern looks different, and instead of producing this hyperarousal (fight/flight response) response, the brain may move towards a “shutdown” or over-modulated state, where higher-order cortical regions, particular areas such as the medial and dorsolateral prefrontal cortex, exert top-down inhibition over the limbic activity. This can dampen the emotional intensity and physiological response, and also reduces an individuals subjective awareness, leading to feelings of detachment, numbness, or unreality.
Dissociation is also closely tied to memory system, particularly the hippocampus and its role in integrating experiences across time. Under high stress, hippocampal functioning can be disrupted, leading to fragmented or state-dependent encoding of memory. This helps explain why dissociative experiences are often associated with gaps in memory, a lack on continuity in autobiographical narrative, and a sense that experiences are not fully “owned” as part of the self.
Another key component involves the brain’s self-referential network, especially the default mode network (DMN), which support a continuous sense of identity. In dissociation, connectivity within and between this network and other regions (e.i., the salient network) can become disrupted. This may contribute to experiences such as depersonalization (feeling detached from oneself) or derealization (feeling detached from the environment), as the brain’s ability to integrate internal and external experience is altered.
Neurochemically, dissociation has been linked to changed in endogenous opioid systems, which can blunt pain and emotional distress, as well as alterations in stress hormones like cortisol. These shifts may further reinforce the “numbing” or distancing feelings associated with dissociation.
From a developmental perspective, these neurobiological patterns build on systems that are already state dependent in childhood. When early environments are unpredictable or overwhelming, the brain may increasingly rely on dissociative pathways as a way to manage distress. Over time, this strengthens neural patterns of disconnection rather than integration, especially in the absence of consistent, regulating relationships.
The neurobiology of Dissociative Identity Disorder (DID) builds on the general mechanisms of dissociation but reflects more chronic, developmentally embedded patterns of compartmentalization across systems involved in identity, memory, and self-processing.
One of the most consistent findings in DID is altered connectivity between brain networks responsible for integrating experience. In particular, disruptions are seen in the default mode network (DMN), which supports a continuous sense of self, and its coordination with the salience network (detecting what is important) and executive control networks (regulation and decision-making). Instead of a cohesive, integrated system, these networks may operate in a more segregated or state-dependent way, contributing to the experience of distinct identity states with differing patterns of awareness, emotion, and behavior.
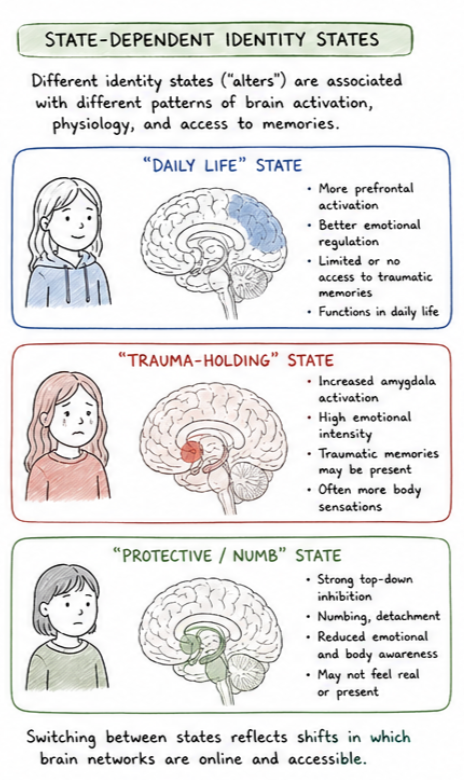
The fronto-limbic system also plays a central role. Studies suggest that individuals with DID show state-dependent changes in activation between the amygdala (threat detection), hippocampus (memory integration), and prefrontal cortex (regulation and inhibition). For example, some identity states may show heightened amygdala activation and hyperarousal, while others show increased prefrontal inhibition and emotional numbing, reflecting alternating patterns of under- and over-modulation of emotion. This aligns with clinical observations of identity states that carry traumatic memories versus those that function in daily life with relative detachment.
Prevalence of Dissociative Disorders
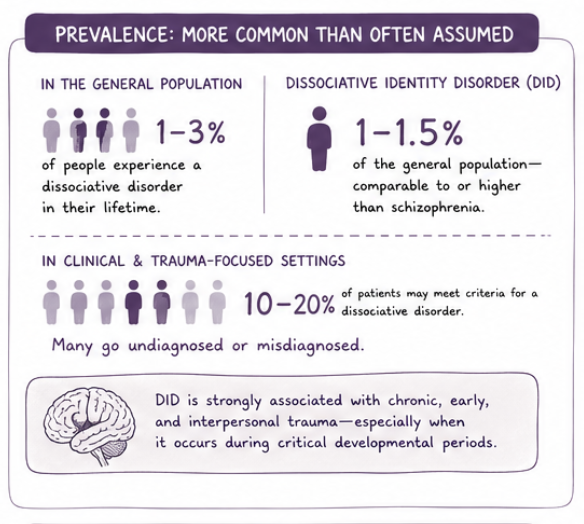
Dissociative disorders are more common than often assumed, particularly in trauma-exposed populations. In the general population, the prevalence of dissociative disorders is estimated to be around 1–3%, with Dissociative Identity Disorder (DID) specifically estimated at approximately 1–1.5%, comparable to or higher than conditions like schizophrenia. Rates are significantly higher in clinical and trauma-focused settings, where studies suggest that 10–20% of patients may meet criteria for a dissociative disorder, though many remain undiagnosed or misdiagnosed. DID, in particular, is strongly associated with chronic, early, and interpersonal trauma, especially when it occurs during critical developmental periods.
Despite this, dissociative disorders are frequently overlooked in trauma-informed care, in part due to limited training, stigma, and the often covert nature of symptoms. Many individuals with dissociation present with depression, anxiety, PTSD, somatic symptoms, or difficulties with attention and emotional regulation, rather than explicitly reporting dissociative experiences. Without recognition, treatment may focus only on surface-level symptoms, which can lead to limited progress or even inadvertent harm (e.g., overwhelming a patient without adequate stabilization).